Glyphosate’s metal-chelating activity causes bioaccumulation of toxic metals in the body, resulting in an estimated 400 000 cases in Sri Lanka and 20 000 deaths Dr Eva Sirinathsinghji
Sri Lanka is set to partially ban glyphosate-based herbicide use following a new peer-reviewed study linking it to a fatal chronic kidney disease epidemic badly affecting the country [1]. Kidney problems have been further documented in other global regions, prompting an earlier complete ban by El Salvador late last year [2]. A complete ban was initially proposed, but due to plantation sector representatives claiming a shortage of agricultural workers that would not sufficiently manage weeds without glyphosate, the government has now limited the ban to disease endemic areas [3]. Even Brazil, one of the largest growers of glyphosate-tolerant genetically modified (GM) crops has now filed a law suit by Federal Prosecutors to ban glyphosate along with 8 other dangerous pesticides [4]. It is becoming increasingly difficult for government regulators and glyphosate producers to justify the use of this herbicide when other nations are banning the chemical outright in order to protect their citizens.
Glyphosate can impact human health in a number of ways, one of which is through its potent metal chelating abilities. Indeed, glyphosate was originally patented by Stauffer Chemical Co. in 1964 (U.S. Patent No. 3,160,632) [5] for this very function. Chelating mineral ions can lead to nutritional depletion in plants and animals, which has already been shown to cause health problems in both. In the case of this kidney disease epidemic, its chelation of metals such as arsenic in the water supplies is now though to lead to their bioaccumulation in the body, resulting in kidney failure and even death, as proposed in a new study [6] by Channa Jayasumana (Rajarata University, Sri Lanka), Sarath Gunatilake (California State University, USA) and Priyantha Senanayake (Hela Suwaya Organization, Sri Lanka) published in the International Journal of Environmental Research and Public Health. Glyphosate has also been linked to many other health problems including cancers (see [7] Glyphosate and Cancer, SiS 62), infertility (see [8] Glyphosate/Roundup & Human Male Infertility, SiS 62), along with neurotoxicity, reproductive problems, birth defects, and other problems (see [9] Ban GMOs Now, special ISIS report).
Starting in the mid-1990s, this Chronic Kidney Disease of unknown aetiology (CKDu) was discovered among the rice paddy farmers in the North Central Province (NCP) of Sri Lanka. Over the next two decades, the disease spread rapidly to the other farming areas. The prevalence of the disease is estimated at 15 % [10] affecting a total of 400 000 patients with an estimated death toll of around 20 000 [11]. The Sri Lankan Ministry of Health have since defined CKDu with the following criteria:
(1) No past history of, or current treatment for diabetes mellitus or chronic and/or severe hypertension, snake bites, urological disease of known aetiology or glomerulonephritis.
(2) Normal glycosylated haemoglobin levels (HbA1C ˂ 6.5%).
(3) Blood pressure ˂160/100 mmHg untreated or ˂140/90 mmHg on up to two antihypertensive agents.
The disease seems to progress slowly, with tubular interstitial nephritis (inflammation of the spaces between renal tubules) associated with mononuclear cell infiltration (infiltration of immune cells – indicative of inflammatory lesions), glomerular sclerosis (hardening or scarring of the renal glomeruli) and tubular atrophy [12]. It is further characterized by tubular proteinurea (excess, unabsorbed protein buildup), usually alpha-1 and beta-2 microglobulinuria proteins, and high urine Neutrophil Gelatinase-associated lipocalin (NGal) levels (>300 ng/mg creatinine).
Different groups including members of the World Health Organisation have already researched the disease and acknowledged a multifactorial cause, with the main causative factors being exposure to arsenic, cadmium and pesticides. Consumption of hard water, low water intake and exposure to high temperatures resulting in significant dehydration, are among the other factors. However, as the authors of the new study state, “whatever hypothesis that is propounded should be able to answer the questions as to why CKDu is confined to certain geographical areas of Sri Lanka and why there was no CKDu in Sri Lanka prior to the 1990s.”
The authors first present a well-documented, statistically significant correlation between water hardness and CKDu. Ninety six percent of the CKDu patients had consumed hard or very hard water for at least five years, which is also clearly illustrated by the maps of Sri Lankan regions showing those most affected by the disease to reside in hard water regions (see figure 1). They also noted further observations in the affected regions:
(a) The number of villagers who complain that the ground water hardness in CKDu endemic area has increased steadily over the last two decades.
(b) Certain shallow wells (2–5 m), previously used for drinking purposes are now abandoned due to high hardness and bad taste.
(c) There are a few natural springs located in the CKDu endemic area where water is not hard. People who consume water from these sources have been determined to be free from the disease.
(d) Individuals who drink treated water from large water supply schemes (especially in the two cities of Anuradhapura and Polonnaruwa), while living in the same endemic areas, do not have the disease.
(e) In the adjoining farming areas of the Northern Province of Sri Lanka, where the ground water hardness level is known also to be hard or very hard, there have not been any significant number of CKDu cases reported.
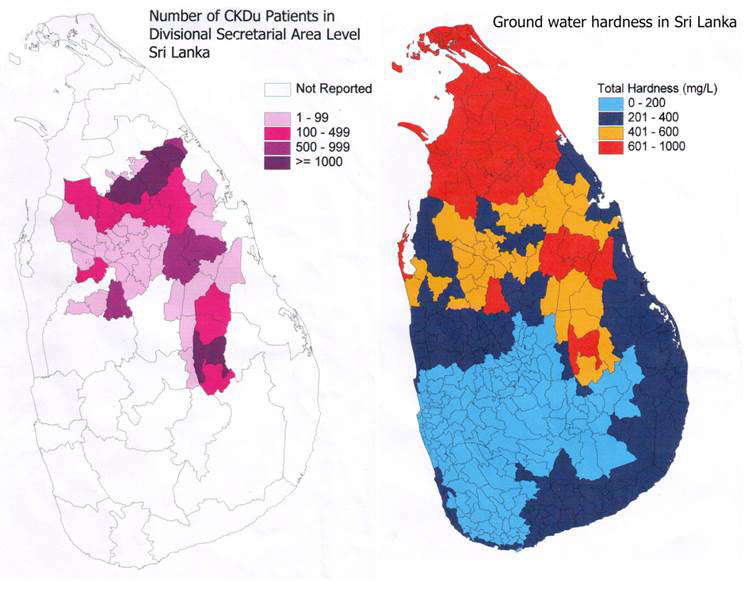
Figure 1 Map of Sri Lanka correlating prevalence of CKDu disease by region (left), with regions of hard or very hard water
Previous evidence has shown that CKDu patients accumulated arsenic in their bodies, with toxic levels of arsenic in urine, hair and nail samples, while healthy people in CDUk endemic regions also show signs of high arsenic levels, suggesting that hard water is linked to CKDu onset [13]. It has been further suggested that the arsenic originates from tainted agrochemicals including pesticides and fertilizers, though the source has not yet been fully determined.
The study reveals that a previously unknown factor, referred to by the authors as ‘compound X’, originates from agrochemicals and that compound X, when combined with hard water containing toxic levels of calcium and magnesium, causes serious kidney damage. In support of the hypothesis that compound X derives from agrochemicals and is indeed glyphosate, are the observations that CKDu emerged in the 1990s, which fits with the massive influx of agrochemicals in Sri Lanka since the 1970s following changes in economic policies. Further, low concentrations can lead to bioaccumulation of a toxic substance, which would explain the 12-15 year lag time before symptoms emerge. This coincides with the shifting age of patients, with prevalence of disease increasing in younger people in recent years, suggesting a cumulative nature of the toxin. In addition, regions of Sri Lanka that have restricted agrochemical use, as in the North where the concern of political, violent conflict meant that governments wanted to prevent people from using agrochemicals to make explosives, high levels of CKDu do not exist. These areas also have hard water, showing that hard water alone is not sufficient to cause CDKu. The authors used these observations to describe the expected properties of compound X listed below:
(a) A compound made of recently (2–3 decades) introduced chemicals to the CKDu endemic area
(b) Ability to form stable complexes with hard water
(c) Ability to capture and retain arsenic and nephrotoxic metals and act as a “carrier” in delivering these toxins to the kidney
(d) Possible multiple routes of exposure: ingestion, dermal and respiratory absorption.
(e) Not having a significant first pass effect when complexed with hard water (a phenomenon of drug metabolism, usually by the liver, whereby the concentration of a drug is greatly reduced before it reaches the systemic circulation)
(f) Presenting difficulties in identification when using conventional analytical methods.
Glyphosate is further implicated by the fact that it is by far the most commonly used herbicide in Sri Lanka, with quantities of glyphosate use exceeding all other pesticides combined.
Glyphosate was first used as a descaling agent to clean out calcium and other mineral deposits from pipes and boilers, aided by the chemical’s high water solubility. Descaling agents bind to metals, making the water soluble and removable. Its stability in water depends on a number of factors, including phosphate which competes with glyphosate for soil absorption. Further, its binding to metals can cause the formation of strong complexes that affect its biodegradability, with glyphosate degradation time increasing to 7-22 years in particular conditions such as pH. In water above pH 6.5, glyphosate turns into a dianion (an anion with a -2 negative charge), suggesting it forms metal complexes in alkaline conditions, increasing its solubility and thus leaching deep into soils [14,15]. Alkaline conditions are known to reduce the weed killing capacity of glyphosate, with glyphosate-metal complexes being stable in basic but not acidic conditions. The effects of pH are also important in understanding the stability of the lattice structure in the acidic conditions of the kidney, as will be explained below.
Studies using nuclear magnetic resonance (NMR) techniques show glyphosate to interact with calcium, magnesium and other metals, and that these complexes become more stable with time [16, 17]. Further, the paddy farming soil in regions endemic for CKDu are rich in metals including calcium, magnesium, iron, nickel, chromium and cobalt. Ferric irons alter soil absorption of glyphosate and its metabolite, AMPA (α-Amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid). This problem is confounded by the application of triple phosphate (TSP) fertiliser to paddy fields, which have been found to be contaminated with certain metal ions as well as high levels of arsenic. This leaves people highly vulnerable to exposure of stable, toxic glyphosate-metal complexes through their drinking water. Glyphosate exposure also occurs through the skin, farmers are found to have glyphosate in urine following spraying. Glyphosate can mix with sweat in hot and humid climates before being absorbed through the skin. Further, Sri Lankan farmers do not often wear protective gear to prevent respiratory exposure. Arsenic and cadmium also commonly contaminate rice, vegetables and tobacco leaves which are often chewed along with betel leaves by Sri Lankans. This transdermal and respiratory exposure therefore provides an additional opportunity for glyphosate to bind to nephrotoxic metals consumed in foods and bioaccumulate in the body.
Based on previously published studies on how glyphosate forms metal complexes and matrices [14-17], the authors propose the formation of stable glyphosate metal lattices, which can explain how glyphosate, hard water, arsenic and other nephrotoxic metals cause kidney disease in Sri Lanka, as well as the increase in water hardness over the years. This proposed glyphosate metal lattice, as shown in figure 2, is based on previous NMR studies showing the ability of hard water ions to bind to both the phosphonate and carboxyl functional groups of the glyphosate molecule to form complexes.
It is worth noting that glyphosate’s causative role in CKDu has previously eluded researchers due to its chemical properties including its ionic character, high polarity, high solubility in water, low volatility, insolubility in organic solvents and strong complexion behaviour, which make it very difficult to detect in the lab.
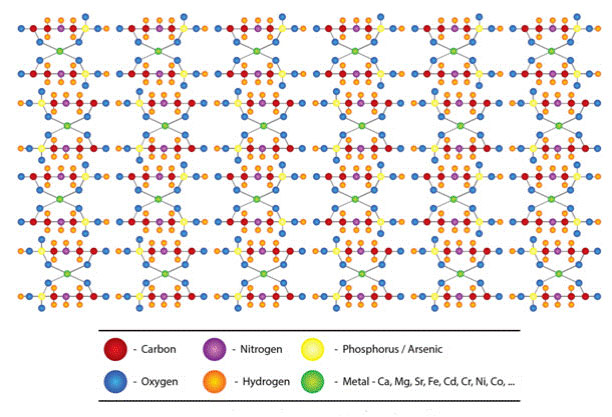
Figure 2 Proposed glyphosate/heavy metal lattice structure
The glyphosate metal lattice hypothesis is supported by the observation that people who drink natural spring water do not suffer the disease, with these waters being devoid of magnesium and calcium, making the water unable to retain glyphosate. It also explains why regions with hard water but low levels of herbicide and chemical fertilizer are free of CKDu. Further, CKDu patients show accumulation of metals (As and Cd) in the hair and nail samples, but low levels of urinary excretion of metals (compared with control subjects in the same regions), suggesting the kidney is unable to properly rid these chemicals from the body. Urine from control as well as CKDu patients in endemic areas also show presence of glyphosate and heavy metals, providing evidence of the presence of components of the glyphosate metal lattice in their bodies. Evidence from El Salvador also points to toxic heavy metals as a culprit in the disease that largely affects poor, agricultural workers in the nation.
The lattice is proposed to accumulate in the kidney where the acidic conditions caused by the daily secretion of acids such as ammonium, cause the breakdown of the lattice. Ammonium sulphate is already used by agriculturalists as a buffer to release glyphosate from metal ions in hard water conditions, suggesting the same mechanism may underlie the effects seen in the kidney proximal tubules in CKDu patients. The lattice breakdown can then release glyphosate and its metabolite AMPA as well arsenic, which may damage the glomeruli. Other heavy metals can then be partially reabsorbed by the kidneys resulting in further tubular damage. Nephrotoxicity of heavy metals is already well known, with long-term exposure causing oxidative stress, nitrosative stress (cell damage caused by reactive nitrogen oxygen species acting together with reactive oxygen species), apoptosis and necrosis in the glomerular and proximal tubular cells [18-21]. Glomerular sclerosis (hardening and inflammation of the kidneys), glomerular collapse and tubular interstitial damage are the result of these pathological mechanisms. Glyphosate alone has also been shown in numerous studies to cause kidney toxicity. Nile Talapia exposed to glyphosate show changes in proximal tubular cells [21]. Exposed juvenile African catfish develop haematopoietic cell death, as well as kidney histopathological changes including dilatation of Bowman’s space (a region of the kidney involved in the first filtration of the blood to form urine) as well as degenerated tubules [22]. Mammalian studies have found increased serum creatinine, blood urea and reduced kidney weight of rats who were fed with glyphosate exposed maize [23]. Oral exposure increases blood urea levels and leads to renal dysfunction in rats [24] while dairy cows suffer similar symptoms [25]. See [9] Ban GMOs Now, ISIS special report, for a comprehensive summary of glyphosate toxicity to health and the environment.
Studies on the effects of glyphosate and hard water metals combined would provide crucial insight into this hypothesis, though there is no publication on this matter despite the known association of glyphosate with such metals.
Other studies have noted alternative mechanisms by which glyphosate can cause kidney damage. Indeed, glyphosate can induce toxicity through a number of mechanisms including the disruption of cytochrome P450 and aromatase pathways that may be responsible for the genotoxic and teratogenic effects seen under glyphosate exposure. A recent review [26] explains how glyphosate has been patented as an antibiotic and shown to kill beneficial gut bacteria in poultry, leading to dysbiosis (microbial imbalance). This may go on to promote the growth of pathogenic bacteria such C.difficile which produce excessive amounts of p-Cresol sulphate, a toxic phenol that is associated with chronic kidney disease and can induce activation of inflammatory cytokines and chemokines, with inflammation playing a key role in kidney disease. Glyhosate also induces a switch from aerobic to anaerobic respiration in E. coli and other gut bacterial species, causing the increased production of indole, a derivative of the aromatic amino acid tryptophan, whose breakdown also requires cytpchrome P450. Tryptophan, an aromatic amino acid whose production depends on the shikimate pathway that glyphosate inhibits, contains an indole ring. Therefore, disruption of trypophan synthesis by gut microbes may well lead to the accumulation of indole in the body. Indole is an important signalling molecule for many bacteria, and along with p-Cresol, is associated with kidney disease.
National governments are beginning to take long overdue steps to protect their citizens from glyphosate, the most commonly used herbicide in the world. Its links to diseases in both humans, crops and livestock can no longer be ignored. Other worldwide governments need to follow the examples of both El Salvador and Sri Lanka in protecting their citizens from a highly toxic chemical.
Article first published 09/04/14
Comments are now closed for this article
There are 4 comments on this article.
Rory Short Comment left 10th April 2014 02:02:38
I think the producers of glyphosate should be charged with crimes against not only humanity but also the biosphere.
John Wilson Comment left 10th April 2014 02:02:46
Might kidney damage be occurring at a slower rate worldwide by the same process. What are the trends in kidney disease globally?
As glyphosate is present in drinking water, food and in the atmosphere we all have traces of glyphosate in our bodies. If glyphosate forms strong nephrotoxic compounds with a range of metals then surely these molecules will be gradually accumulating in nearly everybody - but faster in people who drink hard water and eat food with toxic fertilizer residues.
The first imperative should be to stop all non-agricultural use of glyphosate herbicides.ie. Using it to manage amenity land by local authorities and others. This use of glyphosate does not even have the justification that it is being used to produce food. My local authority, Newcastle City Council, use it extensively on public land.
Dr S K Weragoda Comment left 7th May 2014 16:04:59
I am working on the same issue for three years time. My test results of well water over 1,400 wells through out the country coincide the distribution of CKDu patients will with Fluoride and hardness.
Impact of Fluoride on kidney also well established.
We need to have a national discussion soon as possible to collect all the data and conclude all the relevant causes fro the issue.
My simple idea is that the Compound X would be multifunctional.
Sanjeewa Warnakulasuriya Comment left 12th August 2014 12:12:52
Hi, I'm a resident in Australia and we have been doing charity work to the effected communities with kidny failures. Our next project is to donate a reverse osmosis water purification unit to an identified area in Anuradhapura district.
My question is to Dr S. K. Weragoda and others who have done extencive research on this matter.
Please let me know, donating a water purification plant is the best thing to do or is there any thing else that can be done to benefit wider community. Thanks. Sanjeewa Warnakulasuriya.